
One of the most frustrating realities within the context of Cerebral Palsy (CP) is that "diagnosis", as such, is generally made around the age of 2 years old. In other words, although it may be known that there is SOME level of neurological damage (or at the very least the POSSIBILITY of neurological damage), the "call to action" with respect to a definitive rehabilitation plan is generally deferred until after an official diagnosis is confirmed. To be clear, this is not to say that nothing is being done nor does it mean that best interests are not taken into account...what it does mean, however, is that specific strategies and action plans become significantly more defined and clear once the diagnosis has been made. The logical question people are likely to have after reading that last statement is: what's so strange about that? The answer comes back in the form of another practical question:
Why must we wait until things are so "black" before we act?
In other words, there are many things that can be done within the "grey areas" that do not necessarily require a "diagnosis" in order to confirm viability. Further, the first 12-24 months of life present enormous opportunities to implement profound change due to the high level of neuroplasticity and biomechanical compliance. The need for a diagnosis goes well beyond the practical debate and extends into issues of liability and systemic function of the medical system...to be precise, almost the entire rehabilitation plan is pre-set based on the diagnosis. Although I agree with the necessity for standardization over customization (especially when we are speaking about providing a service to a larger mass of people), it does not mean that there is no room for individual strategies to be formulated that will result in a plethora of tangible (and intangible) positive outcomes.
The next level of questioning is likely to be quite intuitive:
If we don't have a diagnosis, how will we know where to start?
From a broader and more global perspective, we simply need to understand the fundamental reality that, regardless of whether there is a specific pathology involved or not, every human being requires healthy and robust systemic function (vital functions) in order to sustain life. More specifically:
-Respiratory Mechanics
-Lymphatic Function
-Microcirculation (blood and interstitial / intercellular fluid)
Regardless of the diagnosis (or even the presence of a pathology), these are considerations that can be addresses and potentiated in a more immediate fashion. This lends to the "organic" perspective as a precursor to the "mechanistic" perspective. In other words:
The diagnosis establishes the mechanistic strategy ("what is not working and how do we fix it") while early intervention establishes the organic strategy ("what is working and how can it work better").
It should be said that both of these perspective play a role in an effective and efficient rehabilitation strategy...however, the insertion of an organic perspective is what (in my opinion) is generally lacking and even overlooked completely.
Early Detection:
One of my most proud accomplishments with respect to Fascia Therapy is the fact that it addresses these specific "voids" within the strategic options that parents / families / care-givers have. Beyond being a viable "standalone" platform, adjunct / complement, and tactical management strategy, it has a well defined protocol for early detection and intervention.
Over the last 3 years, I have been fortunate enough to work with Dr. Veronica Delgado who is a well known physiatrist and doctor in Chile. She has essentially formulated an "Early Detection Protocol" that uses a simple scoring system to identify potential markers for neurological impairment. In addition (and in conjunction with), I have formulated a specific evaluation protocol that identifies postural and structural markers as well.

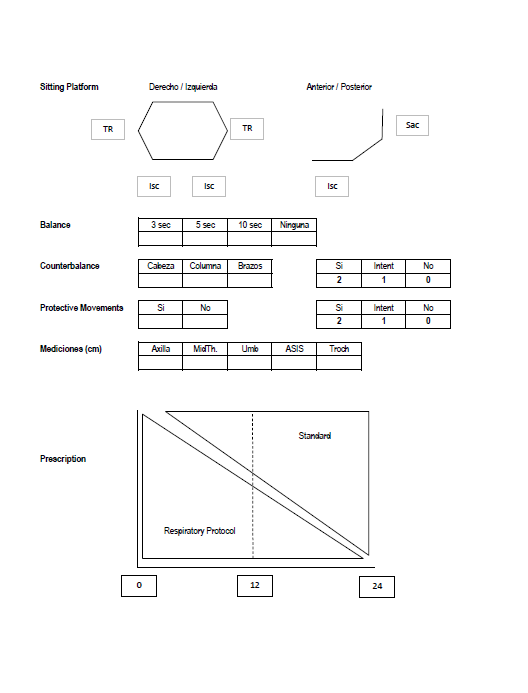
Using both the neurological and structural metrics, we are better able to identify levels risk and therefore set a proper early intervention strategy.
Early Intervention:
As stated earlier, as well in a few of my earlier posts on the importance of respiratory mechanics in neurodevelopmental disorders Part 1 and Part 2 , addressing and potentiating improved respiratory function extends not only into the systemic understanding, but has PROFOUND implications on the development of the pelvis and shoulder girdle...thereby having direct influence on health and function of the hips, legs, and arms. This perspective is something that is worth a read / re-read.
The Fascia Therapy concept addresses this consideration with what is called the Respiratory Protocol which has proven to be a valuable complement to early intervention strategies as well as part of a larger management strategy for all ages with neurological challenges.
Along with the respiratory protocol, there are a group of specialized techniques that potentiate and enhance microcirculation, more specifically interstitial fluid. To put it briefly, interstitial fluid is essentially the medium by which waste product is transported from the bloodstream to the lymphatic system...therefore having a profound impact on systemic health and homeostasis. On addition, immune system function depends greatly on robust interstitial fluid flow. In CP, microcirculation is greatly diminished and effectively manifests in poor tissue quality (colour, texture) as well as overall systemic deficits (chronic illness, stiffness, injury). Being able to properly identify priority "targets" using these techniques greatly enhances systemic homeostasis and ultimately produces a stronger and more resistant organism.
In summary, this post is intended to underscore the reality that, although "black and white" situations do indeed exist, the "grey areas" are exponentially larger...and they should be looked at as opportunities to implement profound, permanent, and lasting improvement.
Cheers!
Gavin
No comments:
Post a Comment